

Cardiovascular Risk Factors in Structural Firefighters
by Marc Clifford, MS, TSAC-F, Darryn Willoughby, PhD, CSCS, FACSM, FACN, FISSN, FASEP, and Craig Hermans, DHSc, TSAC-F, USAW2
TSAC Report
May 2026
Vol 81, Issue 6
This article examines the multifaceted contributors to cardiovascular risk in firefighters and explores targeted interventions to reduce injury and support long-term health.
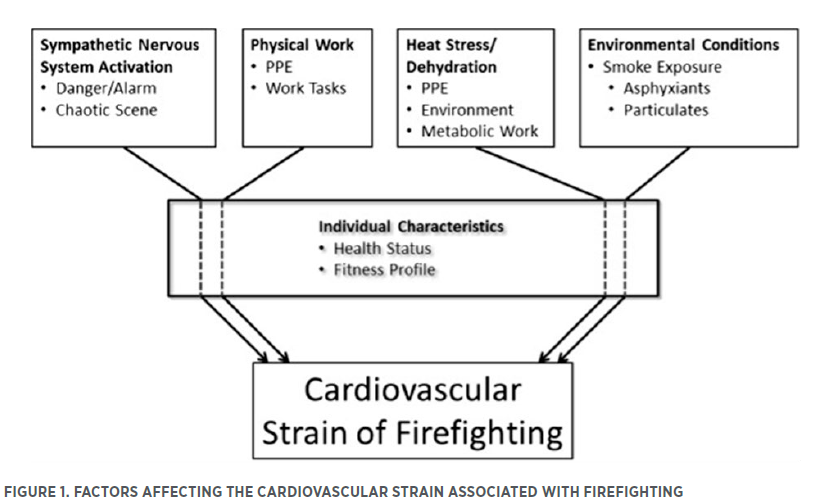
Firefighting is an inherently dangerous and stressful occupation requiring a high level of cardiovascular fitness. However, each year, thousands of structural firefighters are injured or die in the line of duty, with sudden cardiac death (SCD) remaining a leading cause of on-duty fatalities. In 2023, the National Fire Protection Association (NFPA) reported 89 firefighter deaths in the United States, 48 of which were attributed to SCD (7). For every on-duty sudden cardiac death, approximately 17 non-fatal cardiovascular events occur (40). Factors contributing to this risk include obesity, poor nutrition, environmental and thermal stress, sleep deprivation, and a sedentary lifestyle (see Figure 1). This review examines the multifaceted causes of cardiovascular risk among firefighters and suggests potential interventions to mitigate these dangers.
CARDIOVASCULAR RISK FACTORS IN FIREFIGHTERS
SCD is the leading cause of on-duty structural firefighter deaths and a significant cause of mortality in Western countries (4,7,26). SCD in this context is defined as a death occurring within 24 hr of strenuous or stressful on-duty activity (8,26). Common risk factors include obesity, smoking, hypertension, and type 2 diabetes, with obesity showing a powerful association (4). Between 24 – 34% of United States firefighters are classified as obese using body mass index (BMI) standards; however, BMI may overestimate risk in individuals with high muscle mass (29). Nonetheless, the high prevalence of excessive body fat underscores a potentially serious health concern. Firefighters face unique occupational stressors that compound traditional cardiovascular risks. During fire suppression, heart rates can reach close to maximum levels, placing a significant strain on the cardiovascular system (40).
THERMAL AND PHYSIOLOGICAL STRESS
Firefighting exposes workers to extreme heat generated by both fires and the heavy, insulated protective gear required for safety. Firefighting activities have been shown to decrease in stroke volume in the heart and exhibit other signs of cardiac fatigue (14,17,41). The International Society of Sports Nutrition (ISSN) recommends daily water intakes of 2.7 L for women and 3.7 L for men, with electrolyte solutions during operations to replace sweat losses (16). Failure to maintain hydration can reduce cardiac output and oxygen delivery, potentially precipitating infarction and SCD. Sleep deprivation further compounds cardiovascular strain (2). Firefighters often suffer from sleep deprivation (20,28,36,46). Chronic sleep loss increases inflammatory cytokines and disrupts cardiovascular recovery. Combined with sustained physical stress and heat exposure, this creates a potent environment for cardiac dysfunction.
Firefighters are also routinely exposed to environmental toxins through smoke, fuel spills, and chemical incidents. Even their protective gear contains per- and polyfluoroalkyl substances (PFAS) linked to chronic disease (10,18,37). Repeated exposure to such toxins has been associated with long-term cardiovascular and metabolic damage.
PHYSICAL, ENVIRONMENTAL, AND BEHAVIORAL STRESSORS
Firefighting demands prolonged physical exertion in hostile environmental or ambient conditions. Near-maximal effort in extreme heat challenges the body’s ability to maintain perfusion and temperature balance. Protective gear traps heat and sweat, which reduces evaporative cooling and causes dehydration (24,50). As a result, blood viscosity and cardiac afterload are increased. According to Poiseuille’s law, elevated viscosity raises resistance, forcing the heart to work harder to maintain circulation (6,47). This strain, coupled with reduced pulmonary gas exchange, diminishes oxygen delivery and increases the risk of ischemia or infarction—especially in those with preexisting cardiovascular disease (11).
ENVIRONMENTAL EXPOSURE
Firefighters are frequently exposed to polluted air containing fine particulate matter, which has been directly linked to cardiovascular morbidity (1). While single exposures may not cause chronic illness, cumulative exposure dramatically increases disease risk. The World Trade Center disaster exemplified this danger: responders exposed to toxic dust containing cement, metals, and asbestos later developed respiratory and cardiovascular diseases at elevated rates (1,30).
PSYCHOSOCIAL STRESS AND SLEEP DEPRIVATION
Firefighting also imposes heavy psychological burdens. Regular exposure to traumatic events contributes to high rates of depression and post-traumatic stress disorder (PTSD). The US Fire Administration reports suicide rates of 18 per 100,000 among firefighters—higher than the general population—underscoring chronic occupational stress (15). Studies link workplace stress to cardiovascular mortality, arterial stiffness, and impaired sleep quality (9,12,51).
Chronic stress elevates cortisol, a hormone that, in excess, contributes to hypertension, insulin resistance, and adiposity—all risk factors for heart disease (9,19). Increased systemic inflammation, another stress response, promotes atherosclerosis by damaging the vascular endothelium and facilitating plaque deposition (19,29,40). Over time, this process can narrow arteries, increase afterload, and precipitate cardiac events (9,19,29,40).
Sleep deprivation worsens these outcomes. Approximately 73% of firefighters report inadequate sleep during shifts (3). Insufficient rest elevates oxidative stress and inflammatory markers, increasing the risk for cardiovascular disease, obesity, and even cancer (19,34,42,44,48,49). These physiological and psychological stressors interact, amplifying one another and compounding cardiovascular risk.
LIFESTYLE FACTORS AND OCCUPATIONAL CULTURE
Many cardiovascular risks in the fire service stem from modifiable lifestyle behaviors. Despite being classified as tactical athletes, firefighters often mirror the broader population’s health habits—frequently consuming calorie-dense, nutrient-poor foods and leading sedentary lives (24,39).
NUTRITION
Firehouse meals are often communal and centered on convenience, favoring processed foods, red meats, and high-sodium dishes typical of the Standard American Diet (25,39). This dietary pattern contributes to obesity, hypertension, and dyslipidemia. Time constraints, shift work, and unpredictable call schedules contribute to a reliance on such foods. Transitioning toward a Mediterranean-style diet—rich in fruits, vegetables, whole grains, lean proteins, and healthy fats—has been shown to reduce cardiovascular risk and improve lipid profiles (23,31). Education and cultural changes are essential, as food traditions within the fire service are deeply ingrained. Nutrition initiatives and peer-mentoring programs can promote healthier choices without disrupting camaraderie.
PHYSICAL ACTIVITY
Although firefighting requires intermittent intense exertion, many firefighters are sedentary outside of work. Soteriades et al. found that over half of firefighters reported little or no physical activity beyond their job duties (29). This falls short of the World Health Organization’s recommendation of 150 – 300 min of moderate-intensity activity per week (5). Sedentary behavior contributes to obesity, hypertension, and reduced aerobic capacity—all of which elevate cardiovascular risk. Structured fitness programs within departments can improve health outcomes. Aerobic and resistance training enhance cardiorespiratory fitness, lower blood pressure, and improve insulin sensitivity. Exercise also reduces anxiety and depression, providing dual benefits for both physical and mental health.
TOBACCO USE
Tobacco use remains another preventable risk factor. A 2015 national survey found that 21% of firefighters used tobacco—higher than the general US population (21). While cigarette smoking has declined, smokeless tobacco use has increased (35). Both forms are linked to hypertension, atherosclerosis, and cancer. Enhanced cessation programs addressing smokeless tobacco specifically, combined with workplace support and incentives, could significantly reduce this risk.
PREVENTION AND INTERVENTION STRATEGIES
Cardiovascular disease risk factors among firefighters can be categorized into two groups: preventable and non-preventable. Non-preventable risks include genetic predispositions, unavoidable occupational exposures, and inherent elements of sleep disruption associated with shift work. Preventable risks, including diet, exercise habits, and tobacco use, offer the most significant opportunity for improvement.
FITNESS AND EXERCISE
Consistent physical activity is among the most effective ways to mitigate cardiovascular risk (13,38). Regular exercise improves aerobic capacity, reduces fat mass, and enhances resilience to physical stressors encountered on the job (27). Departments should prioritize structured fitness programs, annual assessments, and access to exercise facilities—resources that also demand municipal policies, funding, and experts in tactical strength and conditioning (32). Research consistently shows that physically fit firefighters experience fewer cardiac events and recover more effectively from high-intensity exertion.
NUTRITION AND HYDRATION
Improving nutritional education is equally vital. Implementing wellness programs that teach meal planning, hydration strategies, and the benefits of a Mediterranean-style diet can lead to long-term cultural shifts (23,31). During operations, maintaining hydration with water and electrolyte solutions helps sustain cardiovascular performance and prevent heat-related cardiac strain.
STRESS MANAGEMENT AND SLEEP
Given the psychological toll of firefighting, mental health resources are critical (45). Peer-support teams, counseling services, and mindfulness-based programs can reduce stress and cortisol levels. Departments can also modify shift structures to improve sleep opportunities, such as implementing 48/96 schedules or nap-friendly policies during extended shifts. However, more research is needed in these areas to ensure efficacy.
TOBACCO CESSATION
Comprehensive cessation programs should address both smoking and smokeless tobacco use. Incentive-based approaches, such as reduced insurance premiums or wellness bonuses, may encourage participation (22,33). Departments that integrate cessation support into broader wellness initiatives report higher success rates and improved overall morale (22,33).
CONCLUSION
Firefighting is a noble, yet perilous profession. Beyond the immediate dangers of flames and collapsing structures, firefighters face a silent and pervasive threat—cardiovascular disease. The combination of extreme physical exertion, heat stress, sleep deprivation, poor diet, and occupational exposure creates a perfect storm for cardiac events. However, many of these risks are modifiable. Through structured exercise, improved nutrition, adequate hydration, and tobacco cessation, firefighters can significantly reduce their risk of developing cardiovascular disease. Organizational support, education, and cultural change within departments are key to sustainable success. Resources like the International Association of Fire Fighters (IAFF) and International Association of Fire Chiefs (IAFC) Wellness-Fitness Initiative and the ISSN’s Position Statement on Tactical Athlete Nutrition, Supplementation, and Hydration are good starting points for those looking to implement change within the fire service (16).
Firefighters dedicate their lives to protecting others; by adopting evidence-based wellness strategies, they can better protect their own. Through targeted prevention and intervention, firefighters can transform this high-risk profession into one that not only saves lives but sustains them.
This article originally appeared in TSAC Report, the NSCA’s quarterly, online-only publication geared toward the training of tactical athletes, operators, and facilitators. It provides research-based articles, performance drills, and conditioning techniques for operational, tactical athletes. The TSAC Report is only available for NSCA Members. Read more articles from TSAC Report
References
1. Aryal, A, Harmon, AC, and Dugas, TR. Particulate matter air pollutants and cardiovascular disease: Strategies for intervention. Pharmacology and Therapeutics 223: 2021.
2. Baranwal, N, Yu, PK, and Siegel, NS. Sleep physiology, pathophysiology, and sleep hygiene. ScienceDirect 77: 59-69, 2023
3. Billings, J, and Focht, W. Firefighter shift schedules affect sleep quality. Journal of Occupational and Environmental Medicine 58(3): 294-298, 2016.
4. Bode, ED, Mathia, K, Stewart, D, Moffatt, S, Jack, K, and Smith, D. Cardiovascular disease risk factors by BMI and age in United States firefighters. Obesity (Silver Spring) 29(7): 1186, 2021.
5. Bull, FC, Al-Ansari, S, Biddle, S, Borodulin, K, Buman, M, Cardon, G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine 54(24): 1451-1462, 2020.
6. Cakmak, G, Alkan, F, Korkmaz, K, Saglam, Z, Denizhan, K, Yenigun, M, et al. Blood viscosity as a forgotten factor and its effect on pulmonary flow. Translational Respiratory Medicine 1: 3, 2013.
7. Campbell, R, Hall, S, and Petrillo, J. Firefighter fatalities in the United States: NFPA. June 17, 2024. Retrieved Nov 11, 2024 from https://www.nfpa.org/education-and-research/research/nfpa-research/fire-statistical-reports/fatal-firefighter-injuries.
8. Campbell, R, and Petrillo, JT. Firefighter fatalities in the United States: NFPA. June 11, 2025. Retrieved October 11, 2025 from https://www.nfpa.org/education-and-research/research/nfpa-research/fire-statistical-reports/fatal-firefighter-injuries.
9. Chandola, T, Brunner, E, and Marmot, M. Chronic stress at work and the metabolic syndrome: Prospective study. British Medical Journal 332(7540): 521, 2006.
10. Choi, S, Ekpe, O, Sim, W, Choo, G, and Oh, J. Exposure and risk assessment of Korean firefighters to PBDEs and PAHs via fire vehicle dust and personal protective equipment. Environmental Science and Technology 57(1): 520-530, 2023.
11. Corneanu, LE, Singeap, M, Mutruc, V, Petris, O, Toma, T, Sorodoc, V, et al. The complex relationship between heart failure and chronic obstructive pulmonary disease: A comprehensive review. Journal of Clinical Medicine 14(13): 4774, 2025.
12. Cui, S. Effects and long-term outcomes of endurance versus resistance training as an adjunct to standard medication in patients with stable COPD: A multicenter randomized trial. BMC Pulmonary Medicine 24(1): 196, 2024.
13. Deslandes, A, Moraes, H, Ferreria, C, Veiga, H, Silveira, H, Mouta, R, et al. Exercise and mental health: Many reasons to move. Neuropsychobiology 59(4): 191-198, 2009. https://doi.org/10.1159/000223730.
14. Fernhall, B. Acute effects of firefighting on cardiac performance. European Journal of Applied Physiology 112(2): 735-741, 2012.
15. Firefighter mental health and well-being. 2023. Retrieved 2025 from https://www.usfa.fema.gov/downloads/pdf/summit/2023-factsheets/mental-health-and-wellbeing.pdf.
16. Gonzalez, DE, McAllister, M, Waldman, H, Ferrando, A, Joyce, J, Barringer, N, et al. International Society of Sports Nutrition position stand: Tactical athlete nutrition. Journal of the International Society of Sports Nutrition 19(1): 267-315, 2022.
17. Hibner, BA, Lefferts, E, Yan, H, Horn, G, Smith, D, Rowland, T, et al. Effect of live-fire training on ventricular-vascular coupling. European Journal of Applied Physiology 122(3): 591-597, 2022.
18. IARC Working Group on the Identification of Carcinogenic Hazards to Humans. Occupational exposure as a firefighter. International Agency for Research on Cancer. Retrieved 2025 from http://www.ncbi.nlm.nih.gov/books/NBK597253/.
19. Iob, E, and Steptoe, A. Cardiovascular disease and hair cortisol: A novel biomarker of chronic stress. Current Cardiology Reports 21(10): 116, 2019.
20. Jeong, KS, Ahn, Y-S, Jang, T-W, Lim, G, Kim, H, Cho, S-W. Sleep assessment during shift work in Korean firefighters: A cross-sectional study. Safety and Health at Work 10(3): 254-259, 2019.
21. Jitnarin, N, Poston, W, Haddock, C, Jahnke, S, and Day, R. Tobacco use pattern among a national firefighter cohort. Nicotine and Tobacco Research: Official Journal of the Society for Research on Nicotine and Tobacco 17(1): 66-73, 2015.
22. Jitnarin, N, Poston, W, Jahnke, S, Haddock, C, Kelley, H, and Severson, H. A qualitative study to assess perceptions, barriers, and motivators supporting smokeless tobacco cessation in the US fire service. PLoS One 16(5): e0251128, 2021.
23. Joe, MJ. Dietary behavior and diet interventions among structural firefighters: A narrative review. Nutrients 14(21): 4662, 2022.
24. Kim, S, Kim, D-H, Lee, H-H, and Lee, J-Y. Frequency of firefighters’ heat-related illness and its association with removing personal protective equipment and working hours. Industrial Health 57(3): 370-380, 2019.
25. Kopp, W. How Western diet and lifestyle drive the pandemic of obesity and civilization diseases. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy 12: 2221-2236, 2019.
26. Kumar, A. Sudden cardiac death: Epidemiology, pathogenesis and management. Reviews in Cardiovascular Medicine 22(1): 147-158, 2021.
27. Loewen, B, Melton, B, Ryan, G, and Snarr, R. Evidence-based exercise for structural firefighters—A brief review. TSAC Report 57: 2020
28. Marvin, G, Schram, B, Orr, R, and Canetti, EFD. Occupation-induced fatigue and impacts on emergency first responders: A systematic review. International Journal of Environmental Research and Public Health 20(22): 7055, 2023.
29. Mathias, KC, Bode, ED, Stewart, DF, and Smith, DL. Changes in firefighter weight and cardiovascular disease risk factors over five years. Medicine and Science in Sports and Exercise 52(11): 2476, 2020.
30. Mears, MJ, Aslaner, D, Barson, C, Cohen, M, Gorr, M, and Wold, L. Health effects following exposure to dust from the World Trade Center disaster: An update. Life Sciences 289: 120147, 2021.
31. Mediterranean diet for heart health. Mayo Clinic. July 15, 2023. Retrieved November 13, 2024 from https://www.mayoclinic. org/healthy-lifestyle/nutrition-and-healthy-eating/in-depth/mediterranean-diet/art-20047801.
32. Melton, BF, Ryan, G, Snarr, R, Weeks, M, Langford, E, and Villafuerte, M. Fitness policies within the fire service: A pilot investigation of exercise adherence on fitness outcomes among rural firefighters. American Journal of Lifestyle Medicine 17(3): 437-442, 2021.
33. Nethan, ST, Sinha, DN, Chandan, K, and Mehrotra, R. Smokeless tobacco cessation interventions: A systematic review. The Indian Journal of Medical Research 148(4): 396-410, 2018.
34. Periasamy, S, Hsu, D-Z, Fu, Y-H, and Liu, M-Y. Sleep deprivation-induced multi-organ injury: Role of oxidative stress and inflammation - PMC. 2015. Retrieved November 12, 2024 from https://pmc.ncbi.nlm.nih.gov/articles/PMC4669910/.
35. Phan, L. Trends of cigarette smoking and smokeless tobacco use among U.S. firefighters and law enforcement personnel, 1992–2019. American Journal of Industrial Medicine 65(1): 72, 2021.
36. Ronzani, TM, de Barros, VV, Martins, LF, Saitz, R, and Bastos, RR. Mental health conditions, individual and job characteristics and sleep disturbances among firefighters. Journal of Health Psychology 18(3): 2012.
37. Rosenfeld, PE. Perfluoroalkyl substances exposure in firefighters: Sources and implications. Environmental Research 220: 115164, 2023.
38. Schuch, FB, and Vancampfort, D. Physical activity, exercise, and mental disorders: It is time to move on - PMC. Trends in Psychiatry and Psychotherapy 43(3): 177-184, 2021
39. Simonson, AP, Zera, JN, Banerjee, P, and Baker, BM. Associations between dietary intake and cardiovascular disease risk in American career firefighters: An observational study. Journal of Functional Morphology and Kinesiology 9(3): 132, 2024.
40. Smith, DL, Barr, DA, and Kales, SN. Extreme sacrifice: Sudden cardiac death in the US fire service. Extreme Physiology and Medicine 2: 6, 2013.
41. Smith, DL, Manning, TS, Petruzzello, MS, and Petruzzello, SJ. Effects of live fire training on recruits. Fire Engineering 154(9): 79, 2001.
42. Soteriades, ES. Cardiovascular disease in US firefighters: A systematic review. Cardiology in Review 19(4): 202-215, 2011.
43. Soteriades, ES. Exercise and occupational stress among firefighters. International Journal of Environmental Research and Public Health 19(9): 4986, 2022.
44. Thau, L, Gandhi, J, and Sharma, S. Physiology, Cortisol. Treasure Island, FL: StatPearls Publishing; 2024.
45. The 2nd Alarm Project: Bridging social work and public health to improve mental wellness in the fire service. EBSCO. Retrieved March 8, 2026 from https://research-ebsco-com.zeus.tarleton.edu/c/cl6dr2/viewer/html/o2zncxtgeb.
46. The impact of shift work on the well-being and subjective levels of alertness and sleepiness in firefighters and rescue service workers. 2021. Retrieved March 4, 2026 from https://www.tandfonline.com/doi/abs/10.1080/10803548.2021.1933320.
47. Vincent, J-L. Understanding cardiac output. Critical Care 12(4): 174, 2008.
48. Walker, A, Keene, T, Argus, C, Driller, M, Guy, J, and Rattray, B. Immune and inflammatory responses of Australian firefighters after repeated exposures to the heat. Ergonomics 58(12): 2032-2039, 2015.
49. Watt, PW. Physiological and psychological responses in fire instructors to heat exposures. Journal of Thermal Biology 58: 106-114, 2016.
50. Wohlgemuth, K, Sekiguchi, Y, and Mota, J. Overexertion and heat stress in the fire service: A new conceptual framework. American Journal of Industrial Medicine 66(8):705-709, 2023.
51. Yook, Y-S. Firefighters’ occupational stress and its correlations with cardiorespiratory fitness, arterial stiffness, heart rate variability, and sleep quality. PLoS One 14(12): e0226739, 2019.
Learn about the benefits of NSCA Membership »
About the author
Darryn S. Willoughby, PhD, CSCS
Contact Darryn Willoughby
Your first name is required.
Your last name is required.
Your email is required.
Your message is required.
Your reCaptcha is required.
Your email was successfully sent to Darryn Willoughby
Darryn Willoughby holds a PhD in Exercise Physiology with sub-emphases in Nutritional Biochemistry and Molecular Biology from Texas A&M University. He ...
View full biographyAbout the author
Craig Stephen Hermans, DHSc, MA, TSAC-F
Customer Service, Tarleton State University
craig-hermans-dhsc-usaw-6a8720
Contact Craig Hermans
Contact Craig Hermans
Your first name is required.
Your last name is required.
Your email is required.
Your message is required.
Your reCaptcha is required.
Your email was successfully sent to Craig Hermans
Craig Hermans is a Professional Assistant Professor in the Department of Health and Human Performance at Tarleton State University. He brings over 30 ...
View full biography
Audience:
TSAC Facilitators
TSAC Facilitators
Topics:
Exercise Science Nutrition Exercise Technique Program design Organization and Administration Testing and Evaluation Safety Emergency Procedures Basic Pathophysiology and Science of Health Status or Condition and Disorder or Disease Professional Development
Exercise Science Nutrition Exercise Technique Program design Organization and Administration Testing and Evaluation Safety Emergency Procedures Basic Pathophysiology and Science of Health Status or Condition and Disorder or Disease Professional Development
Keywords:
Firefighters Sedentary Lifestyle Stress Management Occupational Fitness Post-Traumatic Stress Disorder (PTSD) Environmental Exposure Cardiovascular Health
Firefighters Sedentary Lifestyle Stress Management Occupational Fitness Post-Traumatic Stress Disorder (PTSD) Environmental Exposure Cardiovascular Health

- Privacy Policy
- Your Privacy Choices

- Terms of Use
- Retraction and Correction Policy
- © 2026 National Strength and Conditioning Association